

Best PTSD Treatments: 8 Proven Options That Really Help
1) Transcranial Magnetic Stimulation (TMS)
What it is: A non-invasive therapy that uses magnetic pulses to stimulate underactive brain networks linked to mood and fear.
Why it helps: It can lower hypervigilance, reduce intrusive memories, and improve mood—often with minimal side effects.How it works: A small coil rests on your scalp and delivers gentle pulses to the prefrontal cortex. Sessions last ~10 or 20 minutes, 30 sessions over 6 days or 3 to 6 weeks, depending on protocol.
Best for: People who didn’t improve with meds or prefer a drug-free option.
Action steps:Confirm eligibility (metal implants, seizure history, etc.).
Consider pairing TMS with therapy to lock in gains.
Track sleep, mood, triggers weekly.
Learn more: NIMH overview of PTSD care: Traumatic Events and Post-Traumatic Stress Disorder (PTSD

2) Prolonged Exposure Therapy (PE)
What it is: A structured CBT method that reduces fear by safely facing avoided situations and memories.
Why it helps: Avoidance feeds PTSD. PE breaks that cycle.
Format: 8–15 weekly sessions (~90 minutes). Mix of in-vivo exposure (real-life tasks) and imaginal exposure (guided memory processing).
Best for: People ready for a direct, step-by-step plan.
Action steps:
Choose a PE-certified therapist.
Expect short-term discomfort that fades over time.
Do the homework—retrieval practice matters.
Evidence: VA/DoD guidelines list PE as first-line care: PTSD: National Center for PTSD
3) Eye Movement Desensitization & Reprocessing (EMDR)

What it is: A therapy that uses bilateral stimulation (eye movements, taps, tones) to help the brain reprocess stuck trauma memories.
Why it helps: It reduces the emotional charge so you can recall events without intense distress.
Format: 8-phase protocol with preparation, memory targeting, and reprocessing.
Best for: Single-incident trauma or layered histories.
Action steps:
Find an EMDRIA-certified clinician: https://www.emdria.org/
Practice grounding skills between sessions.
Expect vivid dreams or insights as your brain integrates.
4) Trauma-Focused Cognitive Behavioral Therapy (TF-CBT) — for Children & Teens
What it is: A youth-focused CBT model that includes caregivers.
Why it helps: Kids gain coping skills while caregivers rebuild safety and trust at home.
Format: 12–16 sessions (PRACTICE model).
Best for: Children/adolescents with supportive adults.
Action steps:
Work with a TF-CBT-trained therapist.
Caregivers attend sessions and coach skills at home.
Be patient—progress is steady, not linear.
5) Pharmacotherapy
What it is: Prescribed meds—often SSRIs/SNRIs—to reduce core PTSD symptoms (intrusions, hyperarousal, anxiety).
Why it helps: It can stabilize sleep and mood so therapy works better.
Format: Daily dosing; effects build over 4–6 weeks.
Best for: Severe symptoms, sleep issues, or when therapy feels too hard to start.
Action steps:
Track side effects and benefits with your prescriber.
Reassess every 4–8 weeks.
Combine with trauma-focused therapy for best outcomes.
Resource: APA psychedelic info: https://www.apa.org/ptsd-guideline/patients-and-families/psychedelics
6) Narrative Exposure Therapy (NET)
What it is: A brief treatment that organizes your life story and integrates multiple traumas into a coherent timeline.
Why it helps: It replaces fragmented flashbacks with an ordered narrative, reducing distress.
Format: ~4–10 sessions; uses a “lifeline” of flowers (positive events) and stones (traumas).
Best for: Refugees, survivors of organized violence, complex trauma.
Action steps:
Seek a NET-trained clinician.
Build social supports before starting.
Use grounding techniques between sessions.
7) Accelerated Resolution Therapy (ART)
What it is: A fast, directive therapy using eye movements and Voluntary Image Replacement to change the way traumatic images are stored.
Why it helps: You don’t need to retell every detail; you neutralize the charge quickly.
Format: Often 1–5 sessions.
Best for: First responders, military, or anyone wanting a brief, focused approach.
Action steps:
Choose an ART-certified therapist: https://acceleratedresolutiontherapy.com/
Follow directions closely during sessions.
Plan for rapid symptom changes.
8) Somatic (Body-Based) Therapies
What they are: Approaches like Somatic Experiencing and Sensorimotor Psychotherapy that target nervous-system regulation.
Why they help: Trauma lives in the body. These methods resolve fight/flight/freeze patterns and rebuild safety.
Format: Gentle tracking of sensations; titrated exposure; grounding.
Best for: Early/preverbal trauma, dissociation, or when talk therapy stalls.
Action steps:
Work with a certified practitioner (SE, Sensorimotor).
Practice daily grounding (breath, body scans, orientation).
Expect gradual shifts that add up.
Further reading: Van der Kolk’s summary for the public: https://www.nctsn.org/resources/parent-guide-trauma-treatment
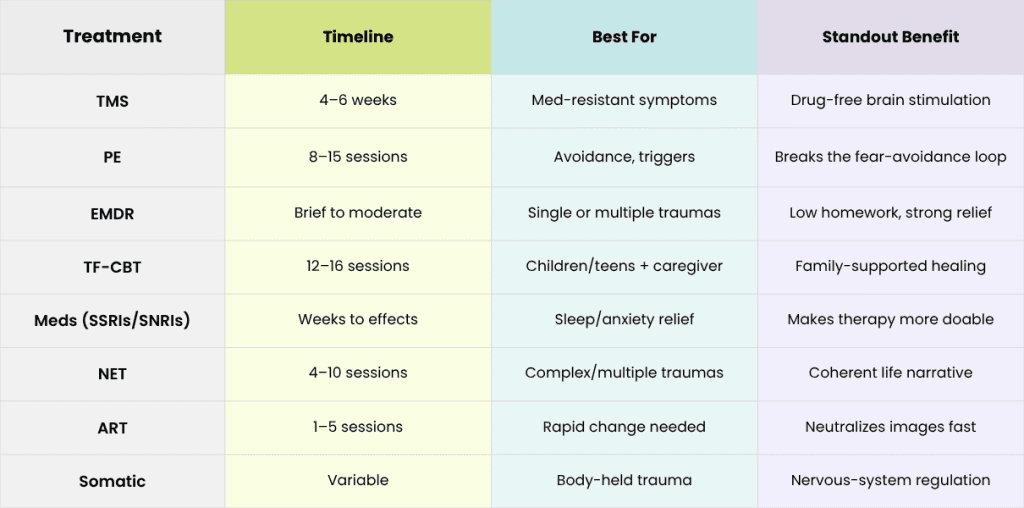
Quick Comparison
How to Choose the Best PTSD Treatment for You
Start with an assessment. A trauma-informed clinician can match treatments to your goals and history.
Combine smartly. Many people pair meds + therapy or mix somatic + cognitive approaches.
Track progress. Log sleep, mood, and triggers weekly. Adjust as needed.
Protect your energy. Healing takes time. Small wins compound.
At BrainStim, we offer innovative, evidence-based options for PTSD, including TMS and integrated care plans. Contact us to discuss next steps.
Recent Research and Developments
The science is always evolving, and recent studies are giving us a clearer picture of ketamine’s long-term impact. Research from 2025 shows a strong link between how long the antidepressant effects last and the amount of neuroplasticity created during the initial treatment phase. On top of that, new evidence suggests that combining ketamine sessions with targeted therapy—right in that “neuroplastic window” after an infusion—can significantly extend the period of symptom relief. It just goes to show how vital an integrated approach really is.
Sources You Can Trust (Outbound)
NIMH PTSD overview: https://www.nimh.nih.gov/health/topics/post-traumatic-stress-disorder-ptsd
WHO stress-related guidelines: https://www.who.int/publications/i/item/9789240003927
VA/DoD PTSD resources: https://www.ptsd.va.gov/
Harvard Health on trauma care: https://www.health.harvard.edu/mental-health
1) Transcranial Magnetic Stimulation (TMS)
What it is: A non-invasive therapy that uses magnetic pulses to stimulate underactive brain networks linked to mood and fear.
Why it helps: It can lower hypervigilance, reduce intrusive memories, and improve mood—often with minimal side effects.How it works: A small coil rests on your scalp and delivers gentle pulses to the prefrontal cortex. Sessions last ~10 or 20 minutes, 30 sessions over 6 days or 3 to 6 weeks, depending on protocol.
Best for: People who didn’t improve with meds or prefer a drug-free option.
Action steps:Confirm eligibility (metal implants, seizure history, etc.).
Consider pairing TMS with therapy to lock in gains.
Track sleep, mood, triggers weekly.
Learn more: NIMH overview of PTSD care: Traumatic Events and Post-Traumatic Stress Disorder (PTSD
2) Prolonged Exposure Therapy (PE)
What it is: A structured CBT method that reduces fear by safely facing avoided situations and memories.
Why it helps: Avoidance feeds PTSD. PE breaks that cycle.
Format: 8–15 weekly sessions (~90 minutes). Mix of in-vivo exposure (real-life tasks) and imaginal exposure (guided memory processing).
Best for: People ready for a direct, step-by-step plan.
Action steps:
Choose a PE-certified therapist.
Expect short-term discomfort that fades over time.
Do the homework—retrieval practice matters.
Evidence: VA/DoD guidelines list PE as first-line care: PTSD: National Center for PTSD
3) Eye Movement Desensitization & Reprocessing (EMDR)
What it is: A therapy that uses bilateral stimulation (eye movements, taps, tones) to help the brain reprocess stuck trauma memories.
Why it helps: It reduces the emotional charge so you can recall events without intense distress.
Format: 8-phase protocol with preparation, memory targeting, and reprocessing.
Best for: Single-incident trauma or layered histories.
Action steps:
Find an EMDRIA-certified clinician: https://www.emdria.org/
Practice grounding skills between sessions.
Expect vivid dreams or insights as your brain integrates.
4) Trauma-Focused Cognitive Behavioral Therapy (TF-CBT) — for Children & Teens
What it is: A youth-focused CBT model that includes caregivers.
Why it helps: Kids gain coping skills while caregivers rebuild safety and trust at home.
Format: 12–16 sessions (PRACTICE model).
Best for: Children/adolescents with supportive adults.
Action steps:
Work with a TF-CBT-trained therapist.
Caregivers attend sessions and coach skills at home.
Be patient—progress is steady, not linear.
5) Pharmacotherapy
What it is: Prescribed meds—often SSRIs/SNRIs—to reduce core PTSD symptoms (intrusions, hyperarousal, anxiety).
Why it helps: It can stabilize sleep and mood so therapy works better.
Format: Daily dosing; effects build over 4–6 weeks.
Best for: Severe symptoms, sleep issues, or when therapy feels too hard to start.
Action steps:
Track side effects and benefits with your prescriber.
Reassess every 4–8 weeks.
Combine with trauma-focused therapy for best outcomes.
Resource: APA psychedelic info: https://www.apa.org/ptsd-guideline/patients-and-families/psychedelics
6) Narrative Exposure Therapy (NET)
What it is: A brief treatment that organizes your life story and integrates multiple traumas into a coherent timeline.
Why it helps: It replaces fragmented flashbacks with an ordered narrative, reducing distress.
Format: ~4–10 sessions; uses a “lifeline” of flowers (positive events) and stones (traumas).
Best for: Refugees, survivors of organized violence, complex trauma.
Action steps:
Seek a NET-trained clinician.
Build social supports before starting.
Use grounding techniques between sessions.
7) Accelerated Resolution Therapy (ART)
What it is: A fast, directive therapy using eye movements and Voluntary Image Replacement to change the way traumatic images are stored.
Why it helps: You don’t need to retell every detail; you neutralize the charge quickly.
Format: Often 1–5 sessions.
Best for: First responders, military, or anyone wanting a brief, focused approach.
Action steps:
Choose an ART-certified therapist: https://acceleratedresolutiontherapy.com/
Follow directions closely during sessions.
Plan for rapid symptom changes.
8) Somatic (Body-Based) Therapies
What they are: Approaches like Somatic Experiencing and Sensorimotor Psychotherapy that target nervous-system regulation.
Why they help: Trauma lives in the body. These methods resolve fight/flight/freeze patterns and rebuild safety.
Format: Gentle tracking of sensations; titrated exposure; grounding.
Best for: Early/preverbal trauma, dissociation, or when talk therapy stalls.
Action steps:
Work with a certified practitioner (SE, Sensorimotor).
Practice daily grounding (breath, body scans, orientation).
Expect gradual shifts that add up.
Further reading: Van der Kolk’s summary for the public: https://www.nctsn.org/resources/parent-guide-trauma-treatment
Quick Comparison
How to Choose the Best PTSD Treatment for You
Start with an assessment. A trauma-informed clinician can match treatments to your goals and history.
Combine smartly. Many people pair meds + therapy or mix somatic + cognitive approaches.
Track progress. Log sleep, mood, and triggers weekly. Adjust as needed.
Protect your energy. Healing takes time. Small wins compound.
At BrainStim, we offer innovative, evidence-based options for PTSD, including TMS and integrated care plans. Contact us to discuss next steps.
Recent Research and Developments
The science is always evolving, and recent studies are giving us a clearer picture of ketamine’s long-term impact. Research from 2025 shows a strong link between how long the antidepressant effects last and the amount of neuroplasticity created during the initial treatment phase. On top of that, new evidence suggests that combining ketamine sessions with targeted therapy—right in that “neuroplastic window” after an infusion—can significantly extend the period of symptom relief. It just goes to show how vital an integrated approach really is.
Sources You Can Trust (Outbound)
NIMH PTSD overview: https://www.nimh.nih.gov/health/topics/post-traumatic-stress-disorder-ptsd
WHO stress-related guidelines: https://www.who.int/publications/i/item/9789240003927
VA/DoD PTSD resources: https://www.ptsd.va.gov/
Harvard Health on trauma care: https://www.health.harvard.edu/mental-health
/ / / / / / / /




Take the Next Step
With clinics across Canada, expert help is closer than you think. Take the first step towards a brighter future today

Navigation
Locations
Support
© 2026 BrainStim. All rights reserved.
Take the Next Step
With clinics across Canada, expert help is closer than you think. Take the first step towards a brighter future today
Navigation
Locations
Framer is a web builder for creative pros. Be sure to check out framer.com to learn more.
Support
© 2026 BrainStim. All rights reserved.

Take the Next Step
With clinics across Canada, expert help is closer than you think. Take the first step towards a brighter future today
Navigation
Locations
Framer is a web builder for creative pros. Be sure to check out framer.com to learn more.
Support
© 2026 BrainStim. All rights reserved.